A common question in advanced pregnancy is: “Has my baby’s head engaged?” Patients are often of the belief that baby’s head must be engaged before they go into labour. That is not true.
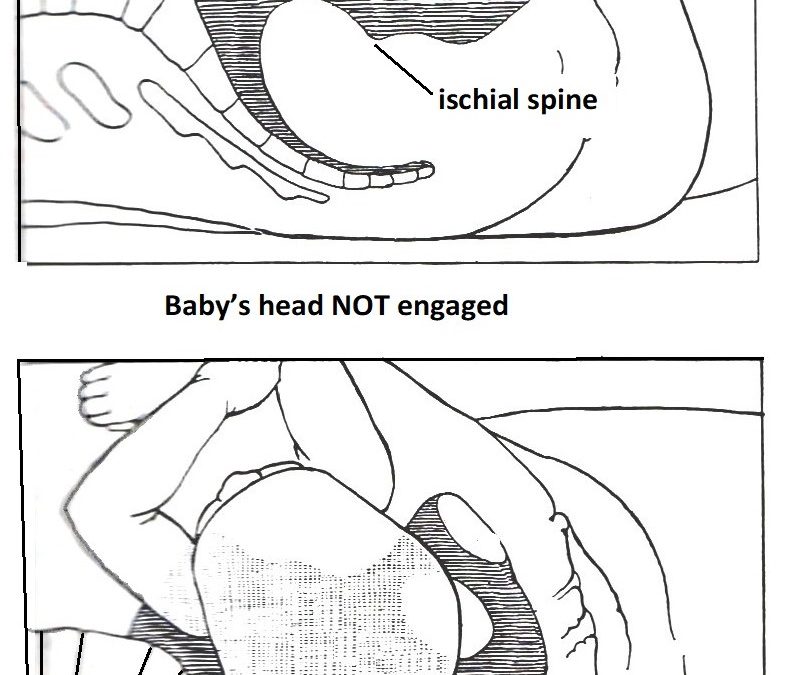
Engagement of baby’s head means the widest diameter of baby’s head (biparietal diameter) has passed through the brim of the pelvis. On abdominal examination an obstetrician can tell as less than ½ of baby’s head can be felt, meaning the majority can’t be felt, as it is in the pelvis. As well, as baby has moved down there is greater gap between the rib cage margin and the top of the uterus. This is called ‘lightening’. The pregnant woman is aware of more heaviness and discomfort in the pelvis and less discomfort at the top of the uterus, easier eating, and less heartburn. On internal examination the top of baby’s head is felt at or below the level of the ischial spines of the pelvis.
While an engaged head is positive sign that labour most likely will start sooner rather than later and that most likely it will be a quicker and more efficient labour, it is not essential for baby’s head to engage before the onset of labour. Baby’s head can be engaged weeks before the onset of labour. Some women when baby’s head is engaged at the outset of labour can have difficult labours.
With ‘multips’ (women who have had a baby or babies) often the baby’s head is not engaged until after the onset of labour. That is because the uterus has been stretched from the first ongoing pregnancy and it is not as snug a space for baby in advanced pregnancy.
While a non-engaged head at the end of pregnancy can be sign that the woman will go overdue. As well if the baby’s head is ‘high’, it can be because her baby’s head is too large for her bony pelvis and/or her baby’s head is deflexed (e.g. occipito-posterior position) and so a larger diameter is presenting.
Last week Kerri-Anne presented at 38 weeks to hospital with spontaneous rupture of membranes but not in labour. It was her third pregnancy. Her first two babies were not delivered by me. Because her labour failed to establish a Syntocinon infusion was commenced. This proven very effective. She as an efficient quick first stage of labour. She did not have an epidural block.
I was contacted by the midwife when her cervix was 9cm dilated because her baby’s heart rate was abnormal, consistent with baby becoming distressed in labour. I had quick check through the remote log in to the birth unit foetal monitor on my computer and agreed. The Syntocinon infusion was ceased. I left the patient who was seeing me in my rooms and immediately went to the hospital. By the time I arrived the abnormal foetal heart rate changes has resolved, and the baby’s heart rate pattern was normal. I did an internal examination and found her cervix to now be fully dilated, but baby’s head was not engaged. It was about 2cm above the ischial spines of her pelvis. Baby’s head was in an occipito-posterior position. I suspected that was the reason baby’s head was high at full cervical dilatation of her cervix.
I encouraged her to push, but only briefly. While she was fully dilated and did not have epidural, she did not have desire to bear down as baby’s head was still high. As the baby’s heart rate pattern was now normal, I asked the midwife to recommence the Syntocinon infusion and so optimise the strength of contractions. I went to the Birth Unit nurses station and waited. I had a cup of tea. There was still no progress and no desire to bear down. The midwife then encouraged her to get off the bed, place her feet on the floor and stand upright resting her hands on the side of the bed. Now with help of gravity and the Syntocinon infusion to strengthen her contractions there was descent of baby’s head and she developed the urge to bear down.
The bearing down sensation intensified. She remined upright in this position resting against the bed.
She was able to push her baby out while being upright. I was squatting behind her with my hands underneath her guiding the delivery of baby’s head. Baby’s head delivered. With another push she delivered baby’s body with my support and into my hands. I passed baby through between her legs to the midwife. The umbilical cord was long enough so baby could be placed on the bed in front of her. The umbilical cord was then clamped and cut. She climbed onto the bed with her baby. I then delivered her placenta by controlled cord traction. There was a first-degree perineal tear which I sutured after injecting local anaesthetic.
Kerri-Anne’s baby’s head did not engage until she was upright in second stage labour. I suspect the reason for this was malpresentation with her baby being in a deflexed occipito-posterior position and so a larger diameter of head presenting. Baby’s head rotated to occipito-anterior position as it descended through the birth canal and delivered as such. As the abnormal CTG’s resolved I suspect they were due to pressure on baby’s head or an episode of compression of baby’s umbilical cord which resolved.
With careful experienced management all worked out well for Kerri Anne and her baby. She is very grateful. Her mother phoned my office to thank me for my good care of her daughter.